Section
11:
Fistulae/Sinuses/Cavities
As with all complex wounds a full assessment to determine the cause and extent of the wound is essential. A fistula is an abnormal passage between a hollow organ and the skin surface, or between two hollow organs¹. “A wound sinus is a discharging blind-ended tract that extends from the surface of an organ to an underlying area or abscess cavity”. The cause of a sinus must always be determined by in-depth assessment. A cavity wound may be chronic or acute and falls into the categories described below.
Treatment options
Fistula

-
Management
and free drainage of exudate.
-
Protection of surrounding skin.
-
Prevention
of infection.
-
Removal of necrosis or slough.
-
Promotion of granulation from the base of the wound.
Hydrogel
Fill
track if exudate is low (using a syringe)
Alginate
or
Fibrous Hydrocolloid
If exudate is moderate to high.
Secondary
Dressing
Foam
or
Soft Silicone Foam
Sinus

-
Allow
cleansing and draining.
-
Do
not plug.
-
Protection of surrounding skin.
-
Prevention of infection.
-
Removal of necrosis or slough.
-
Promotion of granulation from the base of the wound.
Hydrogel
Fill
track if exudate is low (using a syringe)
Alginate
or
Fibrous Hydrocolloid
If exudate is moderate to high.
Secondary Dressing
Foam
or
Soft Silicone Foam
Cavity
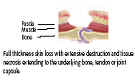
Grade 2

A
cavity wound may be acute or chronic.
Surgical
cavities are generally clean cavities with a healthy bed.
Cavities can be present in a range of aetiologies (pilonidal sinus, pressure ulcers and leg ulcers are examples).
-
Management
and free drainage of exudate.
-
Protection of surrounding skin.
-
Prevention
of infection.
-
Removal of necrosis or slough.
-
Promotion of granulation from the base of the wound.
Hydrogel
Where
there is tracking or undermining.
Alginate
or
Fibrous Hydrocolloid
To fill
cavity.
Fibrous hydrocolloid with foam
For shallow cavities, with moderate to high exudate, if debridement is
required.
Do not occlude.
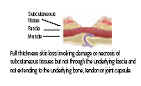
Grade 3
Secondary Dressing
Not required with fibrous hydrocolloid with foam.
Foam
or
Soft Silicone Foam
Grade 4