Section
4: Wound Cleansing
Introduction
There are many different dressing choices for wound management however the
importance of appropriate wound cleansing should not be overlooked. Wound
cleansing is a procedure that has been practised for centuries and is often
considered to be ritualistic and non-evidence based. Rodeheaver and Ratliff
(2007) define wound cleansing as the process required to 'remove surface
contaminants, loose debris, slough, softened necrosis, microbes and/or remnants
of previous dressing from the wound surface and its surrounding skin.'
Wound Cleansing Technique
Irrigation has long been considered one of the most appropriate methods of
cleansing a wound. Irrigation can be achieved using a syringe, pre-filled
irrigation pods or through the patient showering as normal if appropriate.
Cleansing granulating wounds can traumatise new tissue and routine cleansing of
wounds to remove bacteria or to reduce infection is likely to be ineffective
(Allen et al, 2014).
The use of cotton
wool and gauze swabs to cleanse wounds can damage granulating tissue and shed
fibres, which increases the risk of infection.
Cleansing Solutions
For most types of wounds tap water is an appropriate cleansing agent and has not
been found to increase infection rates when compared with sterile water or
saline in recent studies (Fernandez & Griffiths, 2012). In specific wounds that
require aseptic technique such as wounds with exposed bone or tendon, acute skin
tears or wounds in immunocompromised patients, sterile saline should be used.
Scottish Intercollegiate Guidelines Network (2010) recommends using tap water for cleansing chronic leg ulcers. In practice it is preferable to use the patients preferred emollient or Dermol 600 bath emollient mixed with tap water in a lined bucket/basin to cleanse the lower leg. This method also moisturises the surrounding skin and promotes wellbeing in the patient.
Potassium permanganate soaks are recommended for cleansing weeping leg ulcers and further information on how to use this can be found at https://www.dermnetnz.org/topics/potassium-permanganate. Cleansing solutions should be used at body temperature to prevent delayed wound healing. Cooling wounds with cold solutions can delay mitotic cell division for up to three hours (McGuiness et al, 2004).
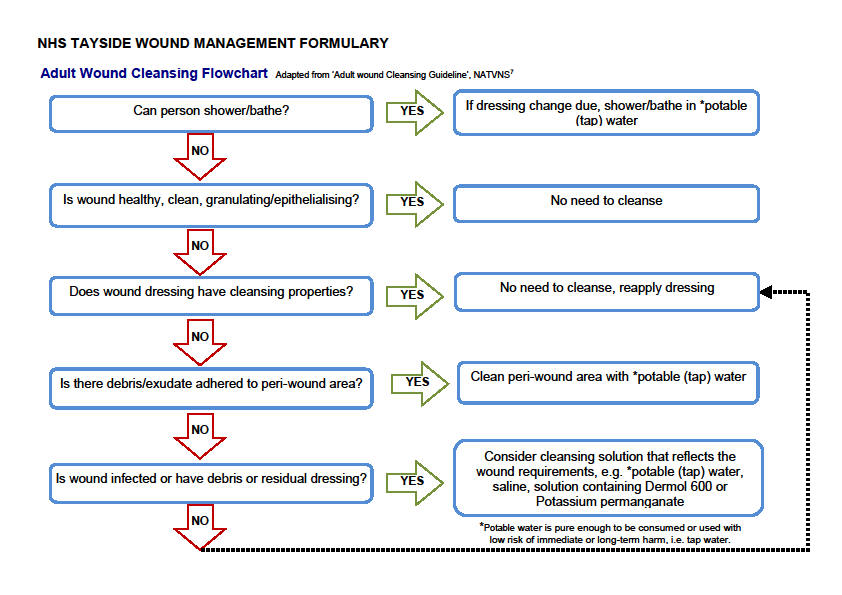
Adult Wound Cleansing Flowchart Adapted from ‘Adult wound Cleansing Guideline’, NATVNS7
References
1 Scottish Intercollegiate Guidelines Network (2010). Management of Chronic Venous Leg Ulcers. SIGN; Edinburgh.
2 Fernandez, R. & Griffiths, R. (2012). Water for wound cleansing. Cochrane Database of Systematic Reviews, Issue 2 Art. No. CD003861.
3 Rodeheaver GT, Ratliff CR (2007) Wound cleansing, wound irrigation, wound disinfection. In: Cutting K (2010) Addressing the challenge of wound cleansing in the modern era. British Journal of Nursing 19(Suppl 11): S24–9.
4 McGuiness, W., Vella, E. & Harrison, D. (2004). Influence of dressing changes on wound temperature. Journal of Wound Care, 13 (9), 383-385.
5 Allen, D., LeBarbera, L.A., Bondre, I.L., Lessing, M.C., Rycerz, A.M., et al (2014). Comparison of tissue damage, cleansing and cross-contamination potential during wound cleansing via two methods: lavage and negative pressure wound therapy with instillation. International Wound Journal 198-209.
6 DermNet NZ website. DermNet New Zealand Trust. Available at: www.dermnetnz.org
7 Adult Wound Cleansing Guideline. NHS Greater Glasgow and Clyde. NATVNS Scotland. Available at: www.tissueviabilityscotland.org/downloads/revisedwoundcleansingflowv5.pdf
Updated: 18 September 2017
© 2010 NHS Tayside